Risk Factors of Depression and Suicidal Behaviors among Adolescents
* Tawima Sirirassamee;
Supakorn Limkhunthummo;
-
* Tawima Sirirassamee: Department of Medicine, Srinakharinwirot University, Thailand.
-
Supakorn Limkhunthummo: Department of Business Administration and Information Technology, Rajamangala University of Technology Suvarnabhumi, Thailand.
-
Mar 16, 2022 |
-
Volume: 1 |
-
Issue: 1 |
-
Views: 1268 |
-
Downloads: 1587 |
Abstract
Objective: To demonstrate the risk factors of depression, suicidal ideation, suicidal attempt and suicide attempt that need hospitalization.
Methods: Data were obtained from the Youth Risk Behavior Survey (2013). This survey was a population based, nationally representative, cross-sectional survey in adolescents aged 13 years to 24-year-old selected by using stratified multistage sampling.
Results: The prevalence of depression, suicidal idea, suicidal attempt, and suicidal attempt that need hospitalization were 10.4%, 2.8%, 2.3%, and 1.1% respectively. The prevalence of suicidal ideation was higher in females than males (2.9% vs. 2.7%), whereas suicidal attempt was higher in males than females (2.5% vs. 2.0%). Low self-esteem, history of sexual abuse, and being cyber bullied were positive predictors both for depression and suicidal ideation. Physical violence exposure and poor academic achievement were positive predictors both for suicidal ideation and suicidal attempt. Heavy alcohol drinking predicted attempt suicide without association with suicidal ideation.
Conclusion: Low self-esteem, exposure to various forms of violence, poor academic achievement, and alcohol drinking were risk factors for suicidal behaviors among Thai adolescents. Suicidal preventive strategy should focus on these factors.
Introduction
Suicide is an important public health problem among adolescents. In United States, suicide is the second leading cause of death after unintentional injury among 15 years to 24-year-old youth [1]. Data from the Thailand Global School Health Survey (GSHS) reported the prevalence of suicidal ideation in the past 12 months was 8.8% (9.9% in males and 7.7% in females) [2]. Previous studies had demonstrated various psychological and environmental factors influence adolescent suicidal behaviors [3]. The 2003 to 2012 GSHS in 32 low-and middle-income countries found that, suicidal ideation was associated with experience of bullying and physical violence, loneliness, limited parental support, alcohol drinking and cigarette smoking [4]. Cyber and physical bullying victimization has been reported to predict adolescent suicide risk [5]. Childhood sexual abuse was demonstrated as a predictor of suicide attempts among depressed adolescents [6]. Data from the Global School Health Survey in African students found the association between suicidal idea and substance abuse (cigarette smoking, alcohol drinking and cannabis use) [7].
Previous study reported the significant positive correlation between suicidal rate and suicidal ideation and suicidal plan in adolescent [8]. However, a study in American students had identified the use of alcohol while sad or depressed as a marker for suicidal behavior in adolescents who did not report ideating prior to an attempt [9]. It is important to determine the precursors that transform the suicidal ideation to suicidal plan and finally suicidal attempted. Identification of high risk adolescents who were more likely to transition from depressed or have suicidal idea to attempt suicide may help in developing the suicide prevention strategy among adolescents. The objectives of this study were to demonstrate the risk factors of depression, suicidal ideation, suicidal attempt and suicide attempt that need hospitalization.
Materials and Methods
Study design and participants
The Youth Risk Behavior Survey (YRBS) was a population based, nationally representative, cross-sectional survey completed between January and March of 2013. Respondents aged 13 years to 24-year-old were selected in the study using a stratified multi-staged sampling. The primary strata consisted of Bangkok and the central, northern, northeastern and southern regions. Two provinces were randomly selected from each of the four regions. Each province was secondarily stratified into urban and rural districts. Households were selected within each cluster using enumeration, followed by a simple random sampling method. A respondent was randomly selected from each household using the “Kish Grid” method [10]. Parents and respondents were asked for formal consent to participate in the survey. Respondents who agreed to participate were instructed to complete the self-administered questionnaire in a private area to ensure privacy from other family members. Ethics approval was granted by Srinakharinwirot University, approval number SWUEC/EX22/2555.
Questionnaire
The 2011 National YRBS is a self-administered questionnaire that has been developed and tested for reliability and validity by the US Centers for Disease Control and Prevention (CDCP) [11]. The questionnaire was translated into the Thai language and reviewed by developmental pediatrician and research team from Mahidol University. The pilot testing was conducted to validate the questionnaire for accuracy and appropriateness. The final Thai version questionnaire contained 75 multiple-choice questions that measured 6 categories of priority health behaviors among youth, which included unintentional injuries and violence, tobacco consumption, alcohol and marijuana consumption, sexual behaviors, dietary behaviors and physical activity.
Measures
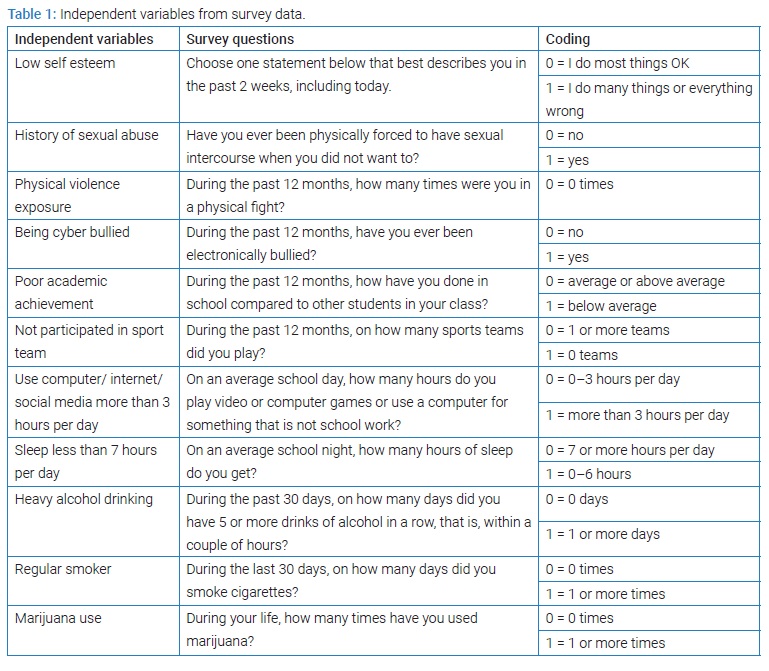
Dependent variables: Four main outcome variables were depression, suicidal ideation, suicidal attempt, and suicidal attempt that need hospitalization. These variables were assessed by four questions asking about feeling and suicide behaviors during the past 12 months. These questions were 1) Did you ever feel so sad or hopeless almost every day for two weeks or more in a row that you stopped doing some usual activities? 2) Did you ever seriously consider attempting suicide or make a plan about how you would attempt suicide? 3) How many times did you actually attempt suicide? 4) If you attempted suicide, did any attempt result in an injury, poisoning, or overdose that had to be treated by a doctor or nurse? The responses for suicidal attempt were 0 times, 1 time, 2 or 3 times, 4 times or 5 times and 6 or more times. The response for others questions were yes or no.
Independent variables: The independent variables derivation from the survey data including low self-esteem, history of sexual abuse, physical violence exposure, being cyber bullied, perceived poor academic achievement, not participated in sport team, use computer or internet more than 3 hours per day, sleep less than 7 hours per day, heavy alcohol drinking, regular smoker, and ever use marijuana were used to determine their predictive effects on the outcome variables. The relevant questions for independent variables and coding are indicated in (Table 1).
Statistical analysis
Descriptive statistics were generated to characterize the samples and to estimate the prevalence of depression and suicidal behaviors. Chi-square analysis was used to describe the independence for gender, age group, and risk factors against depression and suicidal behaviors. The absence of depression and suicidal behaviors associated with risk factors was estimated using odds ratio and was adjusted by gender and age group. Statistical analysis was performed using SPSS version 16.0.
Results
Demographic characteristic
Nine hundred and twenty respondents agreed to participate in this survey and completed the questionnaire. The mean age of the respondents was 18.64 (SD = 3.17) years old. Fifty-six percent of respondents were females and 53.2% were studying in school. The highest proportion of respondents was in the middle adolescent age group (33.9%), followed by late adolescent (33.6%), early adult (24.6%), and early adolescent age groups (7.9%). Ninety seven percent of the respondents were Buddhist. The highest proportion of respondents came from the northeast region (32.2%), followed by the central region (22.1%), northern region (17.3%), southern region (16.7%) and Bangkok (11.7%).
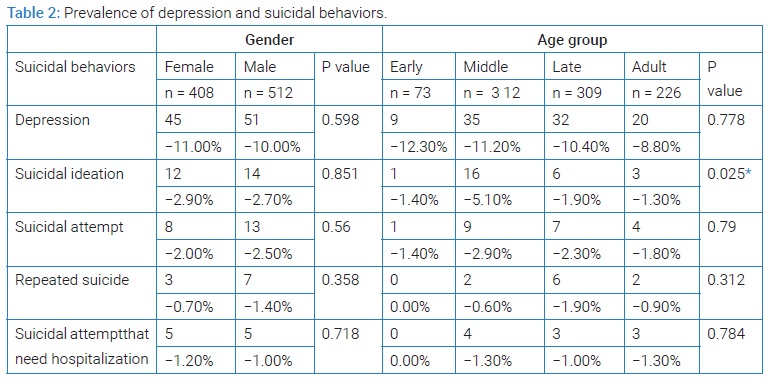
Prevalence of depression and suicidal behaviors by gender and age group
The prevalence of depression and suicide related behaviors. The prevalence of depression, suicidal idea, suicidal attempt, and suicidal attempt that need hospitalization were 10.4%, 2.8%, 2.3%, and 1.1% respectively (Table 2). The prevalence of depression was slightly higher in females than males (11.0% vs. 10.0%) and slightly decreasing in the older age group. The prevalence of suicidal ideation were higher in females than males (2.9% vs. 2.7%), whereas suicidal attempt was higher in males than females (2.5% vs. 2.0%).
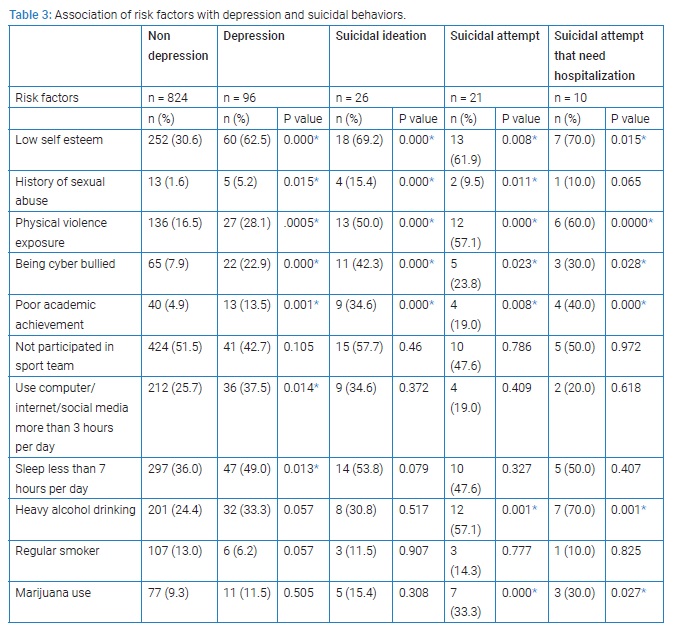
Association of risk factors with depression and suicidal behaviors
The association of risk factors with depression and suicidal behaviors are present in (Table 3). Respondents who reported low self-esteem, being cyber bullied and physical violence exposure and poor academic achievement were significantly associated with depression and all suicidal behaviors. History of sexual abuse was significantly associated with depression and all suicidal behaviors except for suicidal attempt that need hospitalization. Heavy alcohol drinking and ever use marijuana were significantly associated with suicidal attempt and suicidal attempt that need hospitalization but not for depression and suicidal ideation. Excessive use of computer and internet and inadequate sleeping were associated with depression but not for any kind of suicidal behaviors.
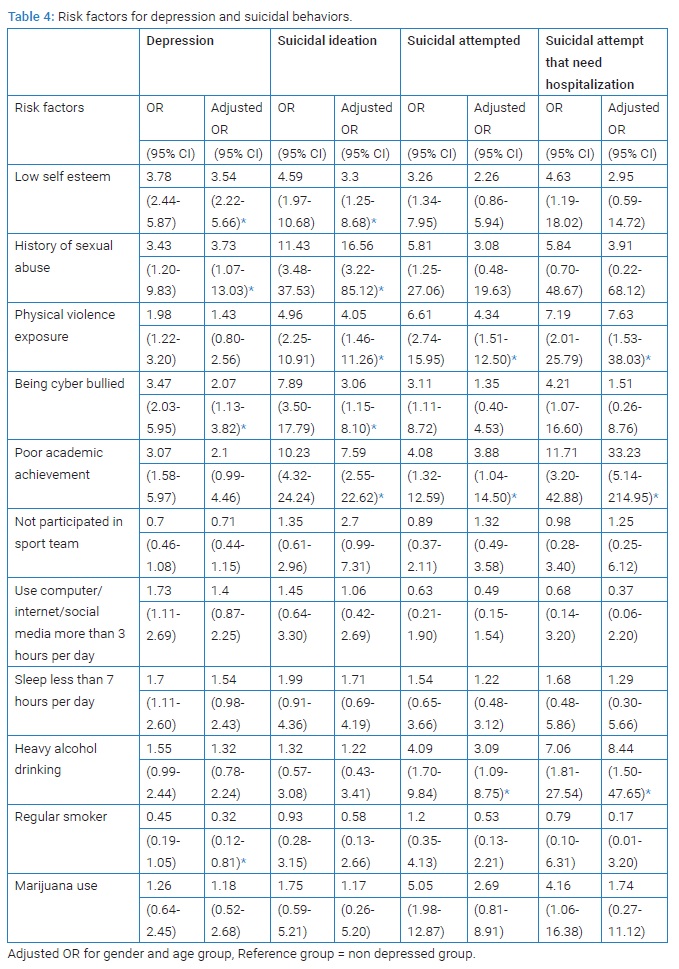
Risk factors for depression and suicidal behaviors
The logistic regression analysis is present in (Table 4). After controlling for sex and age, physical violence exposure and poor academic achievement increases the odds of all suicidal behaviors. Low self-esteem, history of sexual abuse and being cyber bullied increases the odds of depression and suicidal ideation but not for suicidal attempt after adjusting for sex and age. Heavy alcohol drinking increases the odds of suicidal attempt and suicidal attempt that need hospitalization but not for depression and suicidal ideation. Ever use marijuana increases the odds of suicidal attempted and suicidal attempt that need hospitalization but after adjusting for sex and age, the odds were not significantly different.
Discussion
Results from our study found the prevalence of suicidal ideation and suicidal attempt during the past 12 month among. Thai adolescent was 2.8% and 2.3% respectively. A 2003 to 2012 Global School-based Health Surveys among students aged 13 years to 17 years in 32 countries reported that the highest prevalence of suicidal ideation was in African region followed by Region of the Americas, Eastern Mediterranean region and Southeast Asia region. Compared within the Southeast Asia region, the prevalence of suicidal ideation among adolescent in Thailand was lower than those in China and Sri Lanka but higher than Indonesia [4]. Youth risk behavior surveillance - United States reported that the prevalence rate of suicidal attempted during the past 12 months among high school students was increased from 6.9% in 2007 to 7.8% in 2011 [12,13]. A cross-sectional study in 41 schools in England reported that 6.9% of students reported deliberate self harm in the previous year [14]. Recent researchers have identified the similarities and difference between genders in suicidal behaviors. The rate of suicidal ideation and suicidal attempted were consistently demonstrated higher in females than male sin most countries [3,4,15,16]. However, gender difference in suicidal attempt followed by hospital care is still controversy. A 25-year database from the Finnish Hospital Discharge Register (FHDR) reported that 79% of the suicide victims were male [17]. Our results are in line with those found by Roscoat et al. [16], which demonstrated no significant difference in suicidal attempt that need hospitalized between females than males.
In this study, factors that increased risk of both suicidal ideation and suicidal attempt were physical violence exposure and perceived poor academic achievement. Cyber bullying victimization and previous history of sexual abuse were risk factors for suicidal ideation but not significantly increased risk of suicidal attempt. Previous researches have consistently demonstrated the association between bullying and suicide. In the context of the interpersonal theory of suicide, victimization from bullying would represent environmental because thwarted belongingness, perceived burdensomeness, and ultimately suicidal desire. Various factors had been demonstrated as potential mediators that moderated the association between bullying victimization and suicidal behaviors [4,18–22]. Review literature on the association between bullying perpetration, victimization, and suicidal ideation or suicidal attempt, had demonstrated the potential psychological mediators including depression, anxiety, low self-esteem, loneliness, and hopelessness [21]. Similar with those finding, our study found the association between low self-esteem and depression and suicidal ideation. However, low self-esteem did not increased risk for suicidal attempt. The study by Litwiller and Brausch reported that cyber and physical bullying positively predicted suicidal behaviors. Substance use and violence behaviors were partially mediated the relationship between both forms of bulling and suicidal behaviors [18]. Previous research found that verbal and relational bully victimization increased risk for suicide ideation while verbal and physical victimization increased risk for suicide attempt.
This study demonstrate that lower levels of social connectedness and increased severity of bullying involvement as a victim and perpetrator were associated with increased suicide risk [22]. A study in 10 European countries found that physical victimization was associated with suicide ideation while relational victimization was associated with suicide attempt. Low peer and parental support had been identified as a moderator in the association between verbal victimization and suicide behaviors [20]. Our study also found that poor academic perception is a significant predictor of suicidal ideation, suicidal attempt and suicidal attempt that need hospitalization. Those results were similar with a study in 39,542 French adolescents which reported that among suicide attempt in girls, hospitalization was independently predicted by grade repletion [16].
Substances use in this study was alcohol drinking, cigarette smoking, and cannabis using. The results show that alcohol drinking was the only significant predictor of suicidal behaviors. Adolescents who reported heavy alcohol drinking were more likely to attempt suicide but not associated with depression and suicidal ideation. Previous researches indicated that the association between alcohol consumption and suicidal behaviors was inconsistent. Some studies had reported significant association but others did not [8,9,15,23,24]. A 25-year database on suicides from Northern Finland demonstrated that 48% of males and 58% of females were under the influence of alcohol at the time of their suicide [17]. Acute alcohol use can precipitate suicidal behaviors through induction of negative affect and impairment of problem-solving skills, as well as aggravation of impulsive personality traits, possibly through effects on serotonergic neurotransmission [25]. A school-based study in American youth reported that heavy episodic alcohol drinking while down was significantly associated with suicidal attempt among those who did and did not reporting suicidal ideation in the past year [9]. Because there was no sign of depression or suicidal ideation, it is difficult to detect problem prior to their suicidal attempt among this group.
In Mexico, adolescents who used cannabis at early age, cannabis user in the last 12 months and those with heavy cannabis use had increased risk of suicide ideation and attempt [23]. A study in French adolescents reported that among suicide attempt in girls, hospitalization was independently predicted by cannabis smoking [16]. Our study found the association between cannabis use and suicidal attempt but it is not a significant predictor for suicidal behaviors after adjusted for age and sex. This might because of the small number of adolescents who use cannabis in this study. Results from the EU-funded Saving and Empowering Young Lives in Europe (SEYLE) study had reported the association between health behaviors and suicidal behaviors [26]. Frequency of physical activity was negatively correlated with depressive symptoms [27]. Reduced sleep was significant correlated with suicidal ideation [28]. Pathological internet user was significant correlated with depression, suicidal ideation, and suicidal attempt [29]. Contrary to those studies, we did not found the association between participated in sport team, reduced sleep, and excessive use of computer or internet and suicidal behaviors.
This study has few limitations that should be mentioned. Firstly, this was a cross-sectional study, we cannot confidently conclude the causal relationship between risk factors and various stages of suicidal behaviors. Longitudinal study should be done to identify causal correlation. Secondly, data collected in this study were based on self-reports. It is possible that certain risk behaviors were underreported. The survey team tried to minimize under-reporting by stressing the confidentiality of the data.
Conclusion
Three kinds of risk factor for suicidal behaviors has been identifying in this study. Firstly, physical violence exposure and perceived poor academic achievement were the risk factors that increased risk both for suicidal ideation and suicidal attempt. Secondly, heavy alcohol drinking was the risk factor that increased risk of suicidal attempt but did not associated with depression or suicidal ideation. Thirdly, cyber bully victimization and previous history of sexual abuse were the risk factors that associated with depression and suicidal behaviors but not significantly increased risk for suicidal attempt.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- National Center for Health Statistics. National vital statistics system. 2018.
- Peltzer K, Pengpid S. Suicidal ideation and associated factors among school-going adolescents in Thailand. Int J Environ Res Public Health. 2012;9(2):462–473.
- Maslow GR, Dunlap K, Chung RJ. Depression and suicide in children and adolescents. Pediatr Rev. 2015;36(7):299–308.
- McKinnon B, Gariépy G, Sentenac M, Elgar FJ. Adolescent suicidal behaviours in 32 low- and middle-income countries. Bull World Health Organ. 2016;94(5):340–350F.
- Kim YS, Leventhal B. Bullying and suicide. A review. Int J Adoles Med Health. 2008;20(2):133–154.
- Stewart JG, Kim JC, Esposito EC, Gold J, Nock MK, Auerbach RP. Predicting suicide attempts in depressed adolescents: clarifying the role of disinhibition and childhood sexual abuse. J affective disorders. 2015;187:27–34.
- Alwan H, Viswanathan B, Rousson V, Paccaud F, Bovet P. Association between substance use and psychosocial characteristics among adolescents of the Seychelles. BMC Pediatr. 2011;11:85.
- Park S, Jang H. Correlations between suicide rates and the prevalence of suicide risk factors among Korean adolescents. Psychiatry Res. 2018;261:143–147.
- Schilling EA, Aseltine RH, Glanovsky JL, James A, Jacobs D. Adolescent Alcohol Use, Suicidal Ideation, and Suicide Attempts. J Adolesc Health. 2009;44(4):335–341.
- Kish L. A procedure for objetive respondent selection within the household. J Am Stat Assoc. 1949;44(247):380–387.
- Brener ND, Kann L, Kinchen SA. Methodology of the youth risk behavior surveillance system. MMWR Recomm Rep. 2004;53(RR-12):1–13.
- Eaton DK, Kann L, Kinchen S, Shanklin S, Flint KH, Hawkins J, et al. Youth risk behavior surveillance - United States, 2011. MMWR Surveill Summ. 2012;61(4):1–162.
- Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, et al. Youth risk behavior surveillance - United States, 2007. MMWR Surveill Summ. 2008;57(4):1–131.
- Hawton K, James A. Suicide and deliberate self harm in young people. BMJ. 2005;330(7496):891–894.
- Im Y, Oh W-O, Suk M. Risk factors for suicide ideation among adolescents: five-year national data analysis. Arch Psychiatr Nurs. 2017;31(3):282–286.
- Du Roscoät E, Legleye S, Guignard R, Husky M, Beck F. Risk factors for suicide attempts and hospitalizations in a sample of 39,542 French adolescents. J Affect Disord. 2016;190:517–521.
- Lahti A, Harju A, Hakko H, Riala K, Räsänen P. Suicide in children and young adolescents: a 25-year database on suicides from Northern Finland. J Psychiatr Res. 2014;58:123–128.
- Litwiller BJ, Brausch AM. Cyber bullying and physical bullying in adolescent suicide: the role of violent behavior and substance use. J Youth Adolesc. 2013;42(5):675–684.
- Reed KP, Nugent W, Cooper RL. Testing a path model of relationships between gender, age, and bullying victimization and violent behavior, substance abuse, depression, suicidal ideation, and suicide attempts in adolescents. Child Youth Serv Rev. 2015;55:128–137.
- Barzilay S, Klomek AB, Apter A, Carli V, Wasserman C, Hadlaczky G, et al. Bullying victimization and suicide ideation and behavior among adolescents in Europe: A 10-Country Study. J Adolesc Health. 2017;61(2):179–186.
- Hong JS, Kral MJ, Sterzing PR. Pathways from bullying perpetration, victimization, and bully victimization to suicidality among school-aged youth: a review of the potential mediators and a call for further investigation. Trauma Violence Abuse. 2015;16(4):379–390.
- Arango A, Opperman KJ, Gipson PY, King CA. Suicidal ideation and suicide attempts among youth who report bully victimization, bully perpetration and/or low social connectedness. J Adolesc. 2016;51:19–29.
- Borges G, Benjet C, Orozco R, Medina-Mora M-E, Menendez D. Alcohol, cannabis and other drugs and subsequent suicide ideation and attempt among young Mexicans. J Psychiatr Res. 2017;91:74–82.
- Strandheim A, Bjerkeset O, Gunnell D, Bjørnelv S, Holmen TL, Bentzen N. Risk factors for suicidal thoughts in adolescence-a prospective cohort study: the Young-HUNT study. BMJ Open. 2014;4(8):e005867.
- Brady J. The association between alcohol misuse and suicidal behaviour. Alcohol Alcohol. 2006;41(5):473–478.
- Wasserman D. Review of health and risk-behaviours, mental health problems and suicidal behaviours in young Europeans on the basis of the results from the EU-funded Saving and Empowering Young Lives in Europe (SEYLE) study. Psychiatr Pol. 2016;50(6):1093–1107.
- McMahon EM, Corcoran P, O'Regan G, Keeley H, Cannon M, Carli V, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatry. 2017;26(1):111–122.
- Sarchiapone M, Mandelli L, Carli V, Iosue M, Wasserman C, Hadlaczky G, et al. Hours of sleep in adolescents and its association with anxiety, emotional concerns, and suicidal ideation. Sleep Med. 2014;15(2):248–254.
- Wartberg L, Brunner R, Kriston L, Durkee T, Parzer P, Fischer-Waldschmidt G, et al. Psychopathological factors associated with problematic alcohol and problematic Internet use in a sample of adolescents in Germany. Psychiatry Res. 2016;240:272–277.
Keywords
Depression; Suicidal ideation; Suicidal attempt; Risk factors; Suicidal behavior; Adolescent
Cite this article
Sirirassamee T, Limkhunthummo S. Risk factors of depression and suicidal behaviors among adolescents. Glob J Pedia. 2022;1(1):1–7.
