Outcome of Cryomaze Procedure for Chronic Atrial Fibrillation and Re-Connected Lesions of Recurrent Cases
* Takafumi Terada;
Yoshimori Araki;
Akihiro Kobayashi;
Kazuki Sakumoto;
Osamu Kawaguchi;
-
* Takafumi Terada: Department of Cardiac Surgery, JA Aichi Koseiren Toyota Kosei Hospital, Aichi, Japan.
-
Yoshimori Araki: Department of Cardiac Surgery, JA Aichi Koseiren Toyota Kosei Hospital, Aichi, Japan.
-
Akihiro Kobayashi: Department of Cardiac Surgery, JA Aichi Koseiren Toyota Kosei Hospital, Aichi, Japan.
-
Kazuki Sakumoto: Department of Cardiac Surgery, JA Aichi Koseiren Toyota Kosei Hospital, Aichi, Japan.
-
Osamu Kawaguchi: Department of Cardiac Surgery, JA Aichi Koseiren Toyota Kosei Hospital, Aichi, Japan.
-
Aug 07, 2023 |
-
Volume: 2 |
-
Issue: 1 |
-
Views: 1525 |
-
Downloads: 1401 |
Abstract
Objectives: This study aimed to investigate early and late outcomes of the CryoMaze procedure and findings during redo-catheter ablation for recurrent cases.
Methods: We reviewed 51 consecutive patients who underwent the CryoMaze procedure during concomitant cardiac surgery for persistent or longstanding atrial fibrillation between January 2008 and December 2017. We also reviewed the findings of redo-catheter ablation for recurrent cases.
Results: One hospital death was encountered. Sinus rhythm was restored by the end of operation in 31 patients (61%). Thirty-six (72%) and 34 (68%) patients showed sinus rhythm at discharge and 3 months postoperatively, respectively. During follow-up (mean, 30.1 months), 7 late deaths and 3 cases of persisting atrial fibrillation were encountered. Sinus rhythm was restored at least once within 3 months after surgery in 48 cases (including one hospital mortality). In 21 of these 47 patients could be followed after discharge, atrial fibrillation recurred at a mean of 19.4 months postoperatively. Preoperative left ventricle ejection fraction was significantly lower in patients with recurrence. Of the 21 recurrent cases, redo-catheter ablation was attempted for 10 patients. Detected recurrent lesions were a right atrium incision in 1, tricuspid isthmus in 3, mitral isthmus in 4, right upper pulmonary vein in 3, and left upper pulmonary vein in 3, and whole pulmonary veins in 2 patients. All patients were restored to sinus rhythm.
Conclusions: In our series, most patients who underwent the CryoMaze procedure were restored to sinus rhythm. In 44.7% of those patients, atrial fibrillation recurred during follow-up. Sinus rhythm was re-restored in all patients who underwent redo-catheter ablation. Points of recurrence were not located in any specific region.
Abbreviations and Acronyms
AF: Atrial Fibrillation; AT: Atrial Tachycardia; SR: Sinus Rhythm; LAD: Left Atrium Diameter; LVEF: Left Ventricular Ejection Fraction; CABG: Coronary Artery Bypass Grafting; CPB: Cardiopulmonary Bypass; ACC: Aortic Cross Clamp; PM: Pace Maker; RA: Right Atrium; T isthmus: Tricuspid isthmus; M isthmus: Mitral isthmus; RuPV: Right Upper Pulmonary Vein; LuPV: Left Upper Pulmonary Vein; LiPV: Left Inferior Pulmonary Vein; EPS: Electrophysiological Study
Introduction
The Maze procedure was first described as a surgical treatment for Atrial Fibrillation (AF) in 1991 by Cox et al., [1] and became a gold standard for the surgical treatment of AF [2,3]. Because the ‘cut and sew’ technique is difficult to perform, can be time-consuming, and requires cardiopulmonary bypass for an extended period, several modifications have been introduced since its first use.
In 1994, Kosakai et al. [4] reported an alternative technique using cryo-ablation to reduce the atrial incision. This simplified Maze procedure has shown excellent results and has become widespread [5–7].
Bi-polar radiofrequency ablation devices were first described in 1992 and have shown sufficient efficacy to gain acceptance by the majority of cardiac surgeons [8–10]. Although cryothermal methods were reported to be equally effective [11], or more effective [12], in past reports, the majority of institutes have come to use radiofrequency devices.
We have continuously adopted cryo-ablation for the Maze procedure, although surgical ablation devices for the Maze procedure have changed from cryo-ablation to radiofrequency ablation. Catheter ablation for AF has recently been developed widely and some candidates for this method have been cases of recurrence after the Maze procedure. Although AF reportedly recursion 20% to 30% of patients who undergo the Maze procedure, catheter ablation findings, site of recurrence, and site of electrical re-connection lesion have rarely been discussed.
The aims of this study were to investigate early and late outcomes of the CryoMaze procedure and to consider the technical problems involved by reviewing findings from redo-catheter ablation for recurrent cases.
Materials and Methods
We reviewed the clinical charts of 51 consecutive patients who underwent the CryoMaze procedure during concomitant cardiac surgery for persistent or longstanding AF between January 2008 and December 2017. We have also reviewed the findings of redo-catheter ablation for recurrent cases to detect points of recurrent atrial tachyarrhythmia. Patients with paroxysmal AF, patients who underwent left or right atrial maze, pulmonary venous isolation and patients treated using a radiofrequency device were excluded. The clinical data of patients were analyzed, including demographic characteristics, left atrial diameter, preoperative left ventricular ejection fraction, operative procedure and postoperative cardiac rhythm status.
Continuous values were compared using Student’s t-test, Welch’s t-test, or the Mann-Whitney U test, and categorical values were compared by means of the χ2 test or two-sided Fisher’s exact test. Differences were considered significant for values of P < 0.05.
Operative Procedure
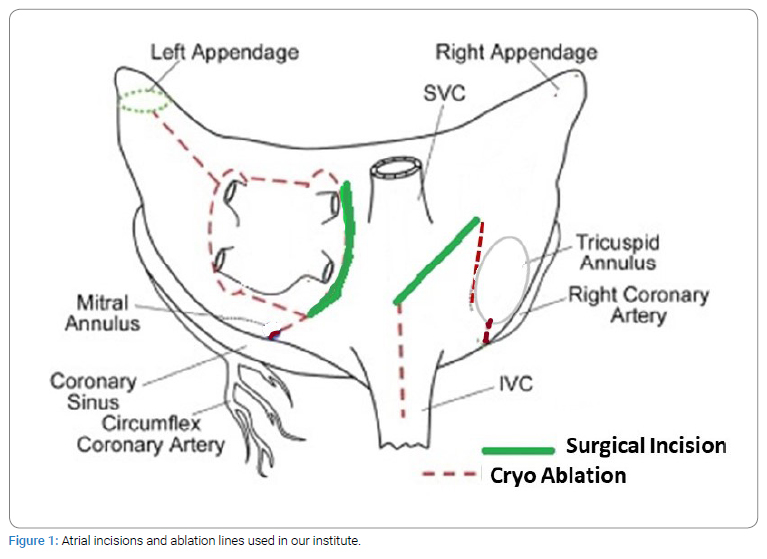
In routine mild hypothermic cardiopulmonary bypass with aortic perfusion and bicaval drainage, all procedures were performed. Cryo-ablation using a Spembly Medical 142 cryo unit (Spembly Medical, Hampshire, UK) was applied for 120 s at -60°C. The atrial incisions and surgical ablation lines used in our institute are shown in (Figure 1).
Results
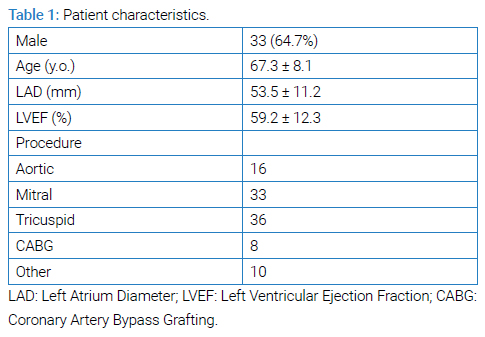
Thirty-three of the 51 patients were male, and mean left atrial diameter and left ventricular ejection fraction were 53.5 mm and 59.2%, respectively (Table 1). As an early postoperative outcome, one hospital death was seen. Operative and postoperative data are shown in (Table 2).
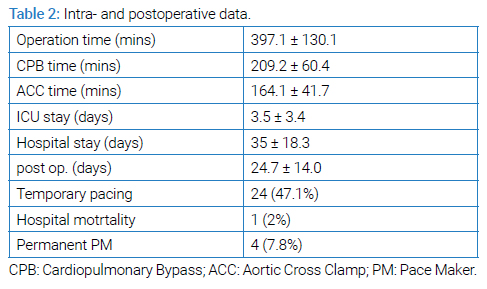
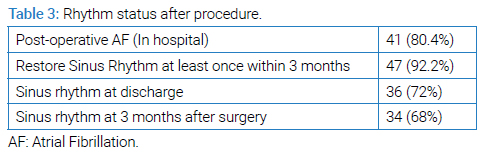
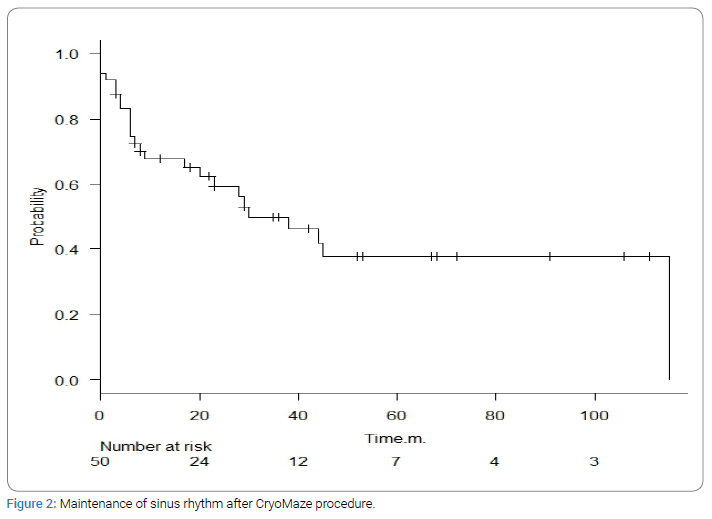
Sinus Rhythm (SR) was restored in 31 patients by the end of the operation and temporary pacing was required in 41 patients during postoperative hospitalization. Although SR was restored at least once after surgery in 48 cases (including one hospital death), AF was documented during the postoperative hospital stay in 41 patients (80.4%). Thirty-six (72%) and 34 (68%) patients maintained SR at discharge and 3 months after surgery, respectively (Table 3). During mean (± standard deviation) follow-up period of 30.1 ± 29.9 months, 7 late deaths were encountered. In 3 cases, AF persisted during whole observation time. In the remaining 48 cases (including one hospital death), SR was restored at least once after surgery. In 21 of 47 patients who restored SR and discharged alive, AF recurred after a mean (± standard deviation) duration of 19.4 ± 24.9 months after surgery (Figure 2).
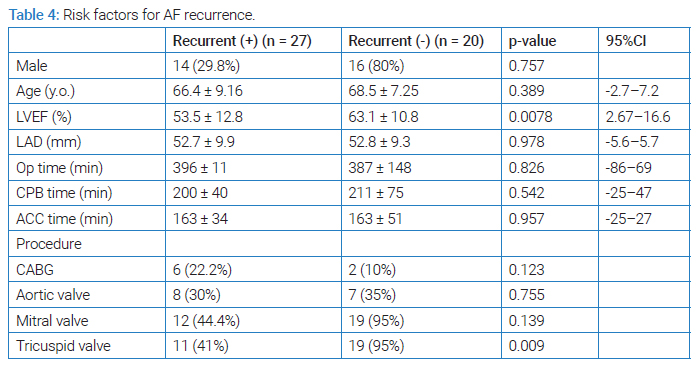
Preoperative left ventricle ejection fraction was significantly lower in recurrent patients than in non-recurrent patients (Table 4).
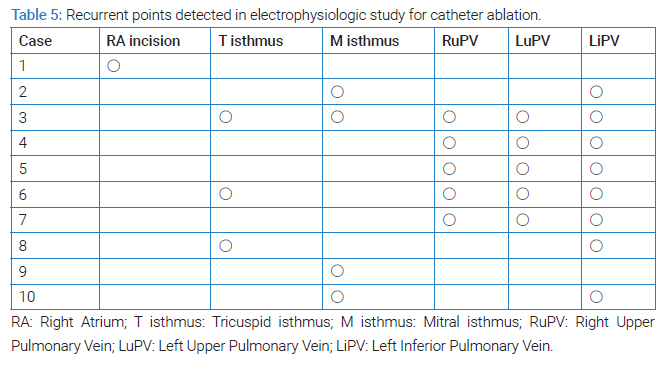
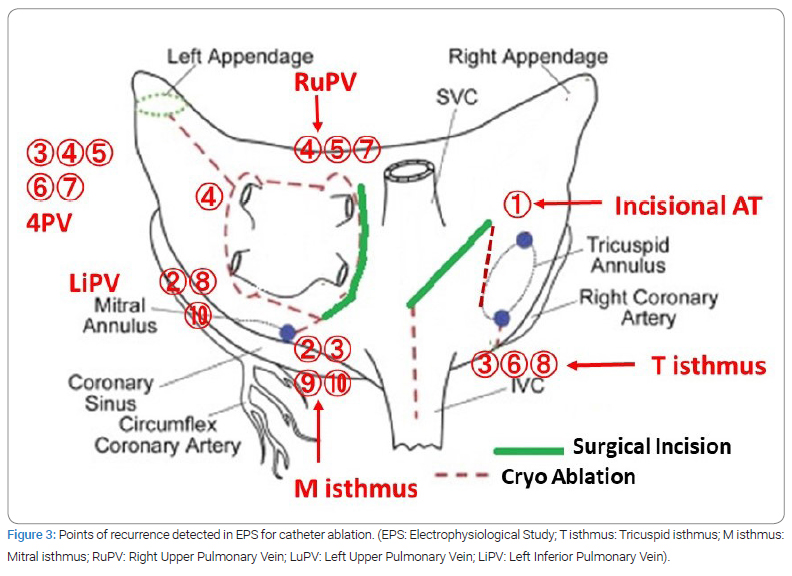
Of the 21 recurrent cases, redo-catheter ablation was attempted for 10 patients. Points at which recurrence of AF was detected were the right atrium incision in 1 case, tricuspid isthmus in 3, mitral isthmus in 4, right upper pulmonary vein in 3, left upper pulmonary vein in 3, and whole pulmonary veins in 2 (Table 5) (Figure 3). All of these 10 patients were restored to SR after redo-catheter ablation.
Discussion
The Maze procedure using cryo-ablation is advantageous for reducing postoperative complications by minimizing incisions and shortening the operative time. These effects of cryo-ablation in the Maze procedure were confirmed in a case-matched study by Nakajima et al. [7].
Whereas the effectiveness of the modified Maze procedure has been confirmed, certain rates of early and late recurrence due to atrial tachyarrhythmias are seen. Early postoperative arrhythmia is common after the maze procedure, and no relationship between incidence of early postoperative atrial arrhythmia and late recurrence of AF has been reported [13]. In our series, SR was restored in 31 patients by the end of the operation and 47 of 51 patients (92.2%) were converted to SR postoperatively. Early postoperative AF was documented 41 patients (80.4%) during the postoperative hospital stay.
The SR conversion rate after the CryoMaze procedure has been reported as 60% to 82% at 12 months after the procedure. As for patients with permanent AF, 47% of patients returned to SR [6].
In this series of patients with persistent or longstanding AF, sinus conversion rates were 92.2% and 68% among patients who maintained SR at 3 months after surgery. Although 92.2% of chronic AF patients returned to SR, AF recurred in 44.7% of these patients during follow-up (mean, 30.1 months). Mean duration from surgery to recurrence was 19.4 ± 24.9 days. In our experience, the CryoMaze procedure was sufficiently effective even against persistent or longstanding AF, whereas the recurrence rate was high in long-term follow-up.
Left ventricular ejection fraction in patients who experienced recurrence of AF after the Maze procedure was significantly lower than that in SR-maintaining patients. Age and left atrial diameter were not significantly different between groups.
With regard to research into AF recurrence after the Maze procedure, published reports have been limited. According to a report by Wazni et al. [14] regarding an electrophysiological study after a ‘cut and sew’ maze, 8 of 23 patients showed recurrent AF secondary to recovered conduction around the lines encircling the pulmonary veins. In a multicenter study of Atrial Tachycardia (AT) after the Maze procedure, 137 patients had 149 ATs that were mapped, with 69% showing a left atrial origin and 31% showing a right atrial origin. Thirty percent had a focal mechanism, and 66% showed an LA origin, with 53% localized to the LA posterior wall. Wide variability in the location of AT circuits was seen in both right and left atria [15]. Electrically re-connected lesions are shown in (Table 5 and Figure 3), with no tendencies seen in our series, as in previous reports. Judging from the fact that most patients were restored to SR from persistent or long-standing AF after surgical maze, recurrent AF seemed to involve restoration of the electrical connection rather than residual electric conduction due to an inadequate procedure.
Most cases of recurrent AF or AT after the Maze procedure were successfully treated using catheter ablation, with a success rate of 93% to 97% [14,15]. In our series, 10 patients underwent catheter ablation for recurrent AF after the Maze procedure. Points of recurrence were detected in all patients and all were restored to SR after redo-catheter ablation.
Limitations
Although this was a single-institution, retrospective observational study, we were able to obtain data over a long follow-up period (maximum 115 months). However, detailed evaluation of recurrent cases should be conducted at other institutions to confirm our findings.
Conclusions
In our series of persistent or long-standing AF, most patients underwent the CryoMaze procedure to restore SR. Although the CryoMaze procedure was effective even for patients with chronic AF, the recurrence rate was high during long-term follow-up.
Although points of recurrence did not appear to be localized to a specific region in catheter mapping, SR was re-restored in all patients who underwent redo-catheter ablation. Catheter ablation may be a feasible option for patients in whom AF recurs after the CryoMaze procedure.
Disclosures
Approval of the research protocol: This retrospective study was confirmed by the Ethics Committee of JA Aichi Koseiren Toyota Kosei Hospital.
Informed consent: All participants provided written informed consent.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
- Cox JL, Schuessler RB, D’Agostino HJ, Stone CM, Chang BC, Cain ME, et al. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991;101(4):569–583.
- Cox JL, Boineau JP, Schuessler RB, Kater KM, Lappas DG. Five-year experience with the maze procedure for atrial fibrillation. Ann Thorac Surg. 1993;56(4):814–824.
- Cox JL, Jaquiss RD, Schuessler RB, Boineau JP. Modification of the maze procedure for atrial flutter and atrial fibrillation. II. Surgical technique of the maze III procedure. J Thorac Cardiovasc Surg. 1995;110(2):485–495.
- Kosakai Y, Kawaguchi AT, Isobe F, Sasako Y, Nakano K, Eishi K, et al. Cox maze procedure for chronic atrial fibrillation associated with mitral valve disease. J Thorac Cardiovasc Surg. 1994;108(6):1049–1054.
- Baek MJ, Na CY, Oh SS, Lee CH, Kim JH, Seo HJ, et al. Surgical treatment of chronic atrial fibrillation combined with rheumatic mitral valve disease: Effects of the cryo-maze procedure and predictors for late recurrence. Eur J Cardiothorac Surg. 2006;30(5):728–736.
- Camm CF, Nagendran M, Xiu PY, Maruthappu M. How effective is cryoablation for atrial fibrillation during concomitant cardiac surgery? Interact Cardiovasc Thorac Surg. 2011;13(4):410–414.
- Nakajima H, Kobayashi J, Bando K, Niwaya K, Tagusari O, Sasako Y, et al. The effect of cryo-maze procedure on early and intermediate term outcome in mitral valve disease: case matched study. Circulation. 2002;106(12 Suppl 1):I46–I50.
- Gaynor SL, Diodato MD, Prasad SM, Ishii Y, Schuessler RB, Bailey MS, et al. A prospective, single-center clinical trial of a modified Cox maze procedure with bipolar radiofrequency ablation. J Thorac Cardiovasc Surg. 2004;128(4):535–542.
- Mokadam NA, McCarthy PM, Gillinov AM, Ryan WH, Moon MR, Mack MJ, et al. A prospective multicenter trial of bipolar radiofrequency ablation for atrial fibrillation: early results. Ann Thorac Surg. 2004;78(5):1665–1670.
- Basu S, Nagendran M, Maruthappu M. How effective is bipolar radiofrequency ablation for atrial fibrillation during concomitant cardiac surgery?. Interact Cardiovasc Thorac Surg. 2012;15(4):741–748.
- Okada M, Usui A, Sakurai T, Terasawa S, Tsunekawa T, Eda T, et al. [Comparative study between cryoablation and radiofrequency ablation for surgical intervention of atrial fibrillation associated with mitral valve disease]. Kyobu Geka. 2010;63(4):297–302.
- Ad N, Holmes SD, Rongione AJ, Massimiano PS, Fornaresio LM. Does surgical ablation energy source affect long-term success of the concomitant cox maze procedure? Ann Thorac Surg. 2017;104(1):29–35.
- Ishii Y, Gleva MJ, Gamache MC, Schuessler RB, Boineau JP, Bailey MS, et al. Atrial tachyarrhythmias after the maze procedure: incidence and prognosis. Circulation. 2004;110(11 Suppl 1):II164–II168.
- Wazni OM, Saliba W, Fahmy T, Lakkireddy D, Thal S, Kanj M, et al. Atrial arrhythmias after surgical maze: findings during catheter ablation. J Am Coll Cardiol. 2006;48(7):1405–1409.
- Gopinathannair R, Mar PL, Afzal MR, Biase LD, Tu Y, Lakkireddy T, et al. Atrial tachycardias after surgical atrial fibrillation ablation: clinical characteristics, electrophysiological mechanisms, and ablation outcomes from a large, multicenter study. JACC Clin Electrophysiol. 2017;3(8):865–874.
Keywords
CryoMaze; Chronic atrial fibrillation; Late recurrence
Cite this article
Terada T, Araki Y, Kobayashi A, Sakumoto K, Kawaguchi O. Outcome of cryomaze procedure for chronic atrial fibrillation and re-connected lesions of recurrent cases. J Heart Disord. 2023;2(1):1–6.
Copyright
© 2023 Takafumi Terada. This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY-4.0).
