* Prashila Amatya: University of California, Riverside School of Medicine, 92521 Botanic Gardens Dr, Riverside, CA 92507, USA.
Chris Mehdizadeh: University of California, Riverside School of Medicine, 92521 Botanic Gardens Dr, Riverside, CA 92507, USA.
Rod Partow-Navid: University of Southern California Keck School of Medicine, 1975 Zonal Ave, Los Angeles, CA 90033, USA.
Ravi M. Rao: University of California, Riverside School of Medicine, 92521 Botanic Gardens Dr, Riverside, CA 92507, USA.
* Ramdas G. Pai: University of California, Riverside School of Medicine, 92521 Botanic Gardens Dr, Riverside, CA 92507, USA.
Jul 17, 2023 |
Volume: 2 |
Issue: 1 |
Views: 1445 |
Downloads: 1528 |
Abstract
A 60-year-old woman presented with nausea, abdominal pain, loss of appetite, and altered mental status. She had an elevated creatine kinase and elevated troponin I that rose from 0.4 ug/dl and peaked at 14.3 ug/dl. Electrocardiogram showed no evidence of ischemic changes, echocardiography showed no wall motion abnormalities, and the patient did not have any chest pain or other concerning cardiac symptoms but had cutaneous manifestations consistent with Dermatomyositis (DM). Cardiac MRI with late gadolinium enhancement revealed focal myocarditis in the left ventricular wall. She was treated with systemic steroids to manage inflammation from DM.
Background
Dermatomyositis (DM) is an uncommon (1–6 in 100,000 patients in the US) autoimmune disease characterized by inflammatory infiltration of the skeletal muscle and skin. Classical symptoms of DM include inflammation of the skin, periorbital edema, and erythema, as well as musculoskeletal findings including proximal weakness, pain, and elevated creatine kinase levels [1]. In many cases DM also exhibits systemic effects, affecting organs such as the lung, gastrointestinal tract, and heart. Cardiac involvement is a significant yet insidious cause of morbidity in DM patients, however no clear mechanism for its development has been elucidated. It is thought that the chronic state of inflammation, as well as prolonged glucocorticoid use in patients receiving treatment, play a role in damaging the myocardium [2]. It is important to suspect myocarditis in a patient presenting with elevated troponin and signs of DM.
Objective
The goal of this case report is to: (1) discuss the differential diagnosis of troponin elevation, (2) stress the importance of a thorough physical examination in the diagnosis and (3) highlight the importance of cardiac MRI to elucidate the mechanism and help direct the right treatment. Transmural distribution of late gadolinium enhancement on Cardiac MRI helps differentiate ischemic versus nonischemic mechanisms and possible cause of nonischemic mechanism.
Case Report
A 60-year-old Hispanic female with hypertension presented to the emergency department with a chief complaint of nausea, abdominal pain, loss of appetite, and altered mental status. Her vitals were normal, but labs revealed an elevated creatine kinase of 3700 U/L, abnormal electrolytes (potassium of 6.1 mmol/L, sodium of 121 mmol/L, chloride of 94 mmol/L) and elevated creatinine of 1.29 mg/dl suggesting acute kidney injury, and a slightly elevated troponin I of 0.411 ug/dl. Echocardiography did not reveal wall motion abnormalities and electrocardiogram did not show evidence of ischemic changes.
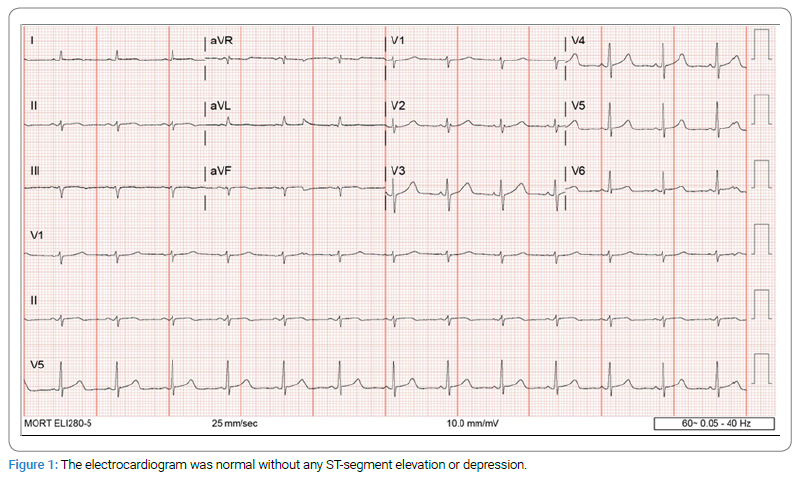
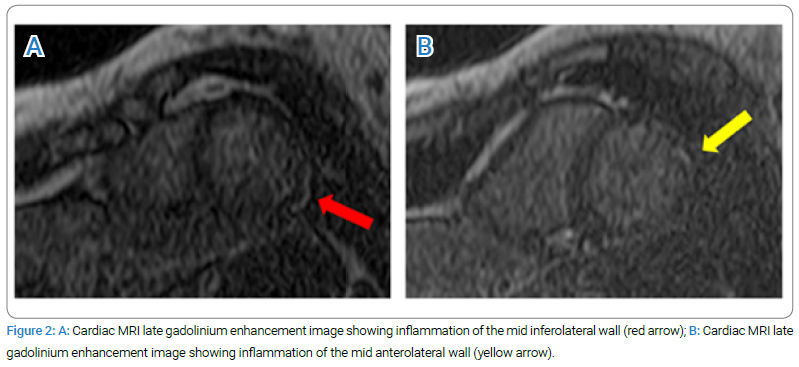
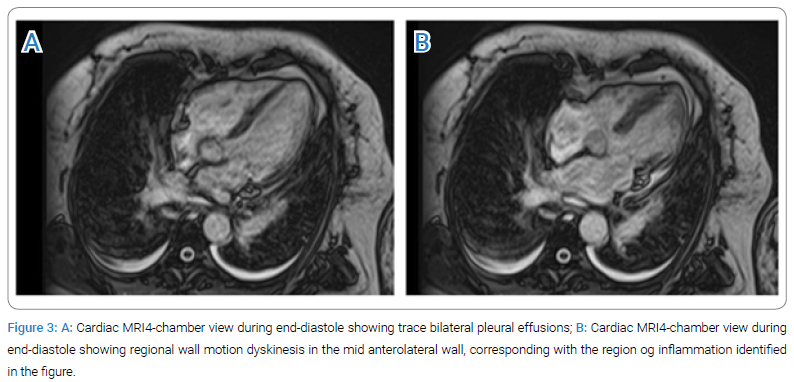
Over the next 48 hours, the patient’s troponin levels continued to rise and peaked at 14.3 ug/dl. She had no chest pain or electrocardiographic abnormalities (Figure 1). The echocardiogram showed normal Left Ventricular (LV) function and the coronary angiogram was normal. The cardiac MRI showed mid-anterolateral left ventricular wall dyskinesis with corresponding areas of delayed enhancement in the mid-myocardial level of the mid-anterolateral wall and sub-epicardial level of the mid-inferolateral wall that were consistent with focal myocarditis (Figure 2A, Figure 2B, Figure 3A and Figure 3B) (Video: Cardiac MRI demonstrating mid-anterolateral left ventricular wall dyskinesis with corresponding areas of delayed enhancement in the mid-myocardial level of the mid-anterolateral wall and sub-epicardial level of the mid-inferolateral wall). The cardiac MRI also demonstrated bilateral trace pleural effusions that could be related to an inflammatory serositis, which would further support our diagnosis (Figure 3A).
The differential diagnoses of acute troponin elevation include acute coronary syndrome, myocarditis and reduced renal clearance due to renal failure. In this patient non-ST elevation myocardial infarction due to epicardial coronary artery occlusion was excluded by coronary angiogram. Myocardial infarction due to coronary microvascular occlusion was made unlikely as the delayed myocardial enhancement was not subendocardial. The midmyocardial or patchy or diffuse enhancement is typical of myocarditis. Subepicardial enhancement is typical of myopericarditis.
Focal transmural enhancement with aneurysms in noncoronary distributions are typically seen in cardiac sarcoid but can occur in other causes of focal myocarditis as well. This patient had 3 distinct types of myocardial enhancements – midmyocardial, subepicardial and focal transmural causing small areas of dyskinesis.
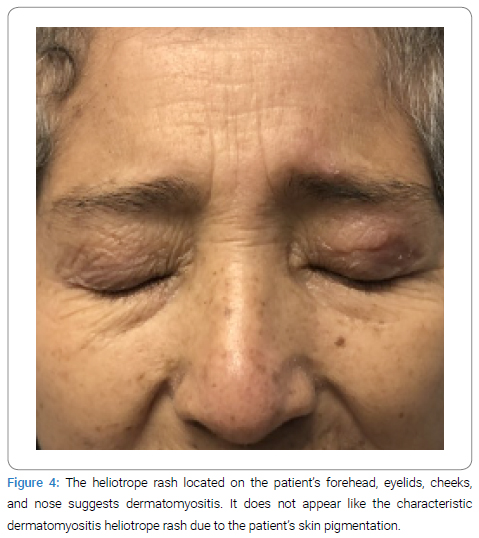
Her symptoms of rhabdomyolysis, proximal muscle weakness, and heliotrope rash pointed towards a diagnosis of dermatomyositis (Figure 4). With the diagnosis of focal myocarditis, the best treatment was to treat the underlying cause, so she was started on systemic steroids for management of dermatomyositis. Troponin I improved to 2.725 ug/dl and creatinine to 0.5 mg/dl. The patient was discharged home on systemic steroids for dermatomyositis.
Video
Discussion
This case involves an uncommon presentation of cardiac involvement in dermatomyositis. Dermatomyositis involves perivascular infiltrates predominated by CD4+ T cells, macrophages, and dendritic cells.The exactpathophysiology of myocarditis secondary to dermatomyositis is unclear; however, histopathology suggests that the same mononuclear inflammatory cell infiltrates localized to perivascular regions of skeletal muscle may affect the myocardium causing cardiomyocyte injury and leading to elevated troponin levels as seen in our patient. Although in this specific case no rhythm abnormalities or symptomatic manifestations occurred, in worse cases myocarditis could affect the cardiac conduction system, cause fibrosis and necrosis of muscle and conductive tissue, or eventually congestive heart failure [2]. Importantly, as occurred in this patient’s case, myocarditis may initially present with elevated troponin similarly to acute coronary syndrome; thus, it is imperative to rule out ischemic causes via EKG and a thorough patient history.
A definitive diagnosis of myocarditis can only be made via endomyocardial biopsy, but cardiac MRI findings such as late gadolinium enhancement and features of edema are highly suggestive of myocarditis. The Lake Louise criteria are widely accepted guidelines for assessment of myocardial inflammation on cardiac MRI [3]. In this case, delayed enhancement and dyskinesis of the left ventricular wall on cardiac MRI in addition to the patient’s systemic inflammatory symptoms and elevated troponin indicated myocarditis.
Cardiac involvement in dermatomyositis has been reported previously. In one case, a 50-year-old Japanese man with no prior diagnosis of dermatomyositis presented with left ventricular hypokinesis and reduced ejection fraction on echocardiography. His troponin was slightly elevated at 0.023 and they chose to conduct a right ventricular endomyocardial biopsy which revealed mononuclear infiltrates with myocyte damage leading to a diagnosis of Clinically Amyopathic Dermatomyositis (CADM). Treatment with prednisolone and tacrolimus led to improved LVEF after 3 months, indicating that the myocarditis may have been related to CADM [4]. In another case, a woman in her 20s diagnosed with dermatomyositis presented with pleuritic chest pain, dyspnea, and elevated troponin levels. Echocardiography showed a hyperdynamic left ventricle and pericardial effusion but no wall motion abnormalities. As in our case, a cardiac MRI was conducted which showed late gadolinium enhancement indicating myocarditis. Treatment with corticosteroids and azathioprine improved her cardiac symptoms [5].
In conclusion, we present an unusual case of DM with myocarditis and focal dyskinesis of the left ventricle. Role of cardiac MRI is emphasized to lead to the right diagnosis and treatment.
Conflict of Interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Informed consent was obtained for this publication.
References
Liu XH, Feng XJ, Shi JY, Jia FW, Liu YX, Zhu YL, et al. The quest for diagnostic approaches of cardiac involvement in polymyositis and dermatomyositis. Ann Palliat Med. 2020;9(4):2256–2270.
Lundberg IE. The heart in Dermatomyositis and polymyositis. Rheumatology. 2006;45(Suppl_4):iv18–iv21.
Sanchez Tijmes F, Thavendiranathan P, Udell JA, Seidman MA, Hanneman K. Cardiac mri assessment of nonischemic myocardial inflammation: state of the art review and update on myocarditis associated with COVID-19 vaccination. Radiol Cardiothorac Imaging. 2021;3(6):e210252.
Kawano H, Kinoshita N, Izumida S, Shimizu T, Umeda M, Maemura K. Myocarditis in a patient with clinically amyopathic dermatomyositis. Circ J. 2020;84(7):1194.
Cheston HJ, Akhoon C, Dutta Roy S, Reynolds P. Managing myocarditis in a patient with newly diagnosed dermatomyositis. BMJ Case Rep. 2022;15(3):e246989.
Amatya P, Mehdizadeh C, Partow-Navid R, Rao RM, and Ramdas G. Pai. A rare cardiac manifestation of dermatomyositis and the importance of cardiac MRI. J Heart Disord. 2023;2(1):1–4.
Infact Publications is the state-of-the-art platform to showcase medical journals across scientific community
and a one-stop solution for publishing the manuscripts of varied medical specialities.
Main Links
Useful Links
Our Contacts
Infact Publications LLC,
16192 Coastal Highway,
Lewes, Delaware 19958 USA